- Research
- Open access
- Published:
Real-world use of over-the-counter medications by patients with migraine in Japan: results from the OVERCOME (Japan) 2nd study
The Journal of Headache and Pain volume 26, Article number: 107 (2025)
Abstract
Background
People with migraine may prefer over-the-counter (OTC) drugs because of multiple reasons, but their overuse can cause medication overuse headaches. This analysis of the ObserVational survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) 2nd study describes the real-world use of OTC headache drugs and the challenges that potentially prevent people with migraine from accessing appropriate medical management in Japan.
Methods
This analysis of the cross-sectional, population-based, nationwide online survey included adults with migraine. Respondents reported their experiences with prescription and OTC drugs for migraine, migraine-specific drug awareness, and attitude towards migraine. Subgroup analyses were performed based on the number of monthly headache days (MHD) and the frequency of OTC drug use/month.
Results
The 19,590 respondents with migraine (68.8% female; mean [SD] age 40.5 [13.1] years) had mean (SD) 3.5 (5.2) MHDs; 29.0% consulted doctors in the past year for migraine. OTC drug use in the past year was common (≥ 62.1%) regardless of doctor consultation or number of MHDs. Among respondents who answered that they would usually use prescribed drugs when they have a migraine attack, 35.2% reported that they would typically use OTC drugs too. The frequency of OTC drug use was the same or higher than that of prescribed drugs in 51.3% of the respondents who consulted doctors in the past year. Only 14.6% of respondents discussed OTC drugs with doctors during consultations in the past year. Migraine-specific drug access and awareness were limited even among frequent OTC drug users (≥ 10 days/month); 18.2% used triptans, but 65.5% never heard of it. Among 37.1% of respondents who had hesitated to visit a doctor, ‘I could handle it myself with OTC medicine’ was the most common reason for hesitation (34.9%).
Conclusion
OTC drug use is common among people with migraine; however, it is not frequently discussed with doctors. Many respondents, even those with frequent OTC drug use, did not have access or awareness of migraine-specific drugs. To prevent medication overuse for migraine, the use of OTC drugs should also be discussed and managed.
Introduction
Migraine is a chronic neurologic disease with a prevalence rate of 7.3–8.4% in Japan [1, 2]. The 2021 Japanese headache guidelines recommend acute treatments for migraine, including over-the-counter (OTC) medications such as acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs) and prophylactic therapy [3]. However, as reported in the ObserVational survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]), 42.6% of patients with migraine do not have adequate access to medical care and appropriate treatment [4].
Patients with migraine may prefer OTC drugs because they are economical and readily available [5], current prescribed drugs result in unsatisfactory outcomes [6], or due to insufficient advanced neurological and headache care and a lack of awareness of proper headache treatment [7]. However, overuse of medications, including OTC drugs, may lead to medication overuse headache (MOH) [8]. The International Classification of Headache Disorders, 3rd edition (ICHD-3) defines MOH as a headache occurring ≥ 15 days/month in individuals with a pre-existing primary headache, developing due to regular overuse of acute or symptomatic headache medications (≥ 10 or ≥ 15 days/month depending on the medication) for > 3 months [9]. In Japan, 2.3–3.7% of patients with migraine may be at risk of MOH [7, 10].
In the real world, clinicians can only understand patients’ OTC drug usage via consultations [11, 12]. However, no matter how clinicians try to capture the exact OTC usage of the patients, there could be limitations as the data are ‘self-reported’. Additionally, OTC drug use is difficult to assess via commonly used real-world data sources such as administrative claims databases because those cannot capture OTC drugs [10]. Therefore, the characteristics, attitudes, and experiences of Japanese patients with migraine who tend to rely on OTC drugs are not well understood.
The OVERCOME (Japan) 2nd study was conducted in 2023, after the approval of new migraine medications in Japan [13], to describe the clinical history, migraine burden, patient-reported outcomes (PRO), and experiences of patients with migraine. This analysis of the OVERCOME (Japan) 2nd study describes the real-world use of OTC drugs among patients with migraine and the challenges that potentially prevent patients from accessing appropriate medical management.
Methods
Study design
Danno et al. [14] explicitly describe the study design of the OVERCOME (Japan) 2nd study. In brief, this observational study was conducted via a cross-sectional, population-based, nationwide online survey in adults with and without migraine. The participants were recruited between June 2023 and August 2023 using survey panels from multiple providers in Japan. After screening, eligible participants were divided into a migraine and non-migraine group. The current analysis was only performed among participants with migraine.
The Medical Corporation TOUKEIKAI Kitamachi Clinic ethics committee approved this study (number BGQ09531) on April 19, 2023. The study was conducted per ethical principles originating from the Declaration of Helsinki and was consistent with Good Pharmacoepidemiology Practices. All applicable Japanese laws and regulations were followed. All survey respondents provided electronic informed consent and agreed to participate in the study. All data were anonymized before analysis. The datasets generated and/or analyzed during the current study are available at Eli Lilly Japan K.K on reasonable request.
Study population and selection criteria
As described previously [14], all participants were ≥ 18 years of age, Japanese residents, had experienced headaches or migraine in the past year, and either self-reported physician-diagnosed migraine or met modified criteria for migraine per International Classification of Headache Disorders – 3rd edition (ICHD-3) criteria [9]. These criteria were validated in the American Migraine Study [15] and the American Migraine Prevalence and Prevention Study [16], as stated in previous OVERCOME studies from Japan [4], the European Union (EU) [17], and the United States (US) [18]. Participants were excluded if all headaches experienced in the past year were secondary headaches caused by hangovers, infections, or trauma; or if inconsistencies were present between the answers to gender and disease.
Variables and outcomes
Participants reported demographic data such as age and sex, clinical characteristics such as the average number of monthly headache days (MHD), the occurrence of probable MOH per ICHD-3 criteria [9] within the past 90 days, and physician consultations over the past year. The impact of migraine was assessed using PRO instruments such as the Japanese Migraine Disability Assessment Scale (MIDAS) questionnaire [19], the Japanese version of the Headache Impact Test-6 (HIT-6) [20], and Migraine Interictal Burden Scale-4 (MIBS-4) [21, 22] (Additional file 1).
Participants also reported their experiences with past and current use of prescription and OTC drugs for migraine, specifically the medications they usually took for migraine attacks. The assessment included monthly medication usage over the past 90 days, any combinations used, triggers for using OTC drugs, awareness about migraine-specific medications, and their attitude towards migraine. Additional file 2 lists the OTC drugs available in Japan for migraine treatment.
Statistical analysis
Data were summarized with descriptive statistics: means and standard deviations (SDs) reported for continuous variables, and frequencies and percentages reported for categorical variables. Subgroup analyses were performed to describe: (a) differences in respondent characteristics and medication use based on the number of MHDs (0–3 MHD, 4–7 MHD, 8–14 MHD, and ≥ 15 MHD i.e. chronic migraine [CM; operational definition based on the data obtainable in the survey]); and (b) differences in respondent characteristics, medical management of migraine, and patient attitudes based on the number of monthly days of OTC drug use (0, 1–4, 5–9, and ≥ 10).
The results were not adjusted for bias and confounding, and statistical comparisons were not performed. Descriptive statistics for categorical and continuous variables were obtained with Python version 3.9.7 (Python Software Foundation) and BellCurve for Excel version 4.04 or later (Social Survey Research Information Co., Ltd., Tokyo, Japan), respectively.
Results
Among the 240,593 eligible respondents for the survey, final analyses were conducted on 19,590 respondents with migraine (Fig. 1). The respondents were stratified into subgroups based on the number of MHDs: 0–3 MHD (n = 14,734), 4–7 MHD (n = 2545), 8–14 MHD (n = 1316), and CM (n = 995); and the number of monthly days with OTC use: 0 days (n = 6806), 1–4 days (n = 10,362), 5–9 days (n = 1267), and ≥ 10 days (n = 1155).

Study participant flow chart
1 Targeted sampling to represent the Japanese adult population in terms of key demographic characteristics (age, sex, and geography) was applied. 2 This included those who passed the screener stage and represented the Japanese census adult population. 3 A quota of 2000 was set for the non-migraine group, and about 2000 respondents were selected from the eligible population while preserving its demographic composition. The majority of respondents eligible for this group were over quota. Abbreviations: CM – Chronic Migraine, N – Total population size, n – Sample size, OTC – Over-the-counter
Demographic characteristics, clinical characteristics, and patient-reported outcomes
The mean (SD) respondent age was 40.5 (13.1) years, and 68.8% were females (Table 1). The majority of respondents met ICHD-3 criteria for migraine (84.9%), but less than half (46.4%) self-reported a physician migraine diagnosis. Respondents experienced a mean (SD) of 3.5 (5.2) MHD at the time of the survey, but only 29.0% (n = 5684) consulted doctors for migraine in the past year. The burden of migraine described in Table 1 has also been reported earlier [14]. Among respondents with probable MOH (2.6%) (Table 1), combination analgesics-overuse headache (56.5%) and NSAIDs-overuse headache (34.6%) were the most common MOH subtypes (Additional file 3).
The migraine subgroups (0–3 MHD, 4–7 MHD, 8–14 MHD, and CM) had generally similar mean age and gender distribution (Table 1). The 8–14 MHD and CM subgroups had high proportions of respondents with a self-reported physician migraine diagnosis (≥ 53.8%). In the MHD subgroups, an increase in the number of MHDs showed a trend of greater respondent burden and doctor visits.
Subgroup analysis by frequency of OTC drug use showed that respondents with ≥ 5 monthly days of OTC drug use had numerically more MHDs and greater migraine-related burden than respondents with ≤ 4 monthly days of OTC drug use (Additional file 4). The ≥ 10 monthly days of OTC drug use subgroup had the highest proportion of respondents with probable MOH (29.6%).
OTC and prescription drug use
The majority of the respondents had ever used OTC (84.4%) or prescribed acute drugs (56.6%) in the past, but preventive drug use was low (25.7%) (Table 2). Prescribed acute drug use in the past year and current preventive drug use were numerically greater among respondents who consulted doctors for migraine in the past year (83.2% and 36.0%) compared with the overall population (42.6% and 13.4%). On the other hand, OTC drug use in the past year was numerically lower in this subpopulation compared with the overall population (65.6% vs. 72.7%). An increase in the number of MHDs showed a trend of greater use of prescribed acute and preventive drugs in the overall population and subpopulation who consulted doctors for migraine in the past year (Table 2).
The frequency of acute drug use in total, including both prescribed and OTC drugs, was numerically greater among respondents who consulted doctors for migraine in the past year than in the overall population (mean [SD] number of days/month 6.8 [8.7] vs. 3.8 [6.5]) (Fig. 2a and b). The frequency of prescribed acute drug use showed the same trend (4.8 [7.9] vs. 1.8 [5.2]). On the other hand, the frequency of OTC drug use was similar among respondents who consulted doctors for migraine in the past year and the overall population (mean [SD] number of days/month 2.5 [5.1] vs. 2.2 [4.4]). The proportion of respondents whose frequency of OTC drug use was equal to or more than that of prescribed acute drug use was lower in respondents who consulted doctors in the past year than in the overall population (51.3% vs. 79.0%) (Fig. 2a and b).

Monthly use of prescribed acute and OTC drugs. (a) Overall respondents with migraine and (b) Respondents who consulted doctors for migraine in the past year. The stacked bar chart corresponds to the left Y-axis and the black line graph corresponds to the right Y-axis. In the survey, respondents answered ‘number of days of drug use’ separately for each individual drug. The counts were summed up to obtain the total reported here for each of the summed number of days of any prescribed acute drug use and summed number of days of any OTC drug use. We reported this in the table, as well as in the stacked bar chart. The respondents also separately answered the number of days of any acute drug use (including both OTC and prescribed drugs); this is only shown in the table below the graph. The sum of number of days of ‘OTC drug use’ and number of days of ‘any prescribed acute drug use’ is not equal to ‘any acute drug use’, because multiple drugs may have been used in combination on the same day. Abbreviations: CM – Chronic Migraine, MHD – Monthly Headache Days, N – Total population size, n – Sample size, NSAID – Non-steroidal Anti-inflammatory Drug, OTC – Over-the-counter, SD – Standard Deviation
The average frequency of any acute, prescribed acute, and OTC drug use/month numerically increased with greater MHD subgroups in the overall population and the subpopulation who consulted doctors for migraines in the past year (Fig. 2a and b). The proportion of respondents whose frequency of OTC drug use was equal to or more than that of prescribed acute drug use was highest in the 0–3 MHD subgroup (81.7% and 55.4%). This proportion was 66.7% and 39.5% in the CM subgroups of the overall population and subpopulation, respectively.
The survey also asked respondents what acute drugs they would usually use when they had migraine attacks. Here too, respondents who consulted doctors for migraines in the past year would usually use prescribed acute drugs more than the overall population (62.3% vs. 32.7%) (Table 3). The use of each prescribed drug class, namely triptans, NSAIDs, and acetaminophen, showed the same trend. On the other hand, the proportion of OTC drug use was numerically lower in those who consulted doctors in the past year compared with the overall population (53.6% vs. 75.2%).
Among respondents in the overall population who would usually use prescribed acute drugs for their migraine attacks, 35.2% answered that they would also use OTC drugs (Table 3). This proportion was similar (31.3%) in the subpopulation who consulted doctors in the past year. When evaluated by each class of prescribed acute drug that the respondents would usually use, the use of any OTC drug in addition to a triptan (27.1% and 26.3%), an NSAID-containing OTC drug in addition to a prescribed NSAID (39.9% and 36.3%), and an acetaminophen-containing OTC drug in addition to a prescribed acetaminophen (11.0% and 13.6%), was similar in the overall population and the subpopulation who consulted doctors in the past year, respectively.
Respondents’ medical management, experience, and awareness of migraine-specific drugs
Most respondents (74.3%) never used preventive drugs for migraine, while 43.4% never used prescribed acute drugs (Table 4). Herbal medicine (9.4%) and NSAIDs or acetaminophen (42.9%) were the most used preventive and prescribed acute drugs, respectively. Use of migraine-specific drugs (calcitonin gene-related peptide monoclonal antibodies [CGRP mAbs] and ditans [both 2.2%], and triptans [13.5%]) was low.
Subgroup analysis by frequency of OTC drug use showed that, even among respondents with ≥ 10 monthly days of OTC drug use, as many as 28.8% had never visited a doctor (Table 4). Moreover, 65.8% and 35.7% of respondents in this subgroup never used preventive and prescribed acute drugs, respectively. Use of CGRP mAbs increased with greater frequency of OTC drug use, but no clear trend was observed in triptan and ditan usage.
The majority of the respondents (73.1–89.9%) had never heard of migraine-specific drugs (triptans, CGRP mAbs, and lasmiditan) (Table 4). Awareness of these drugs was numerically higher among respondents with ≥ 5 monthly days of OTC drug use (13.1–34.5%) than in those with ≤ 4 monthly days of OTC drug use (9.2–29.2%). Among the respondents who consulted doctors for migraine in the past year, 46.4% were not aware of triptans, but the majority had never heard of CGRP mAbs (76.4%) or lasmiditan (78.0%; Table 2).
Respondents’ communication with doctors and attitude toward medical consultation for migraine
Among respondents who had experienced consultations with a doctor for their headaches, 37.1% had ever hesitated in the past to visit a doctor (Table 5). This proportion tended to increase with greater frequency of OTC drug use. ‘I could handle it myself with OTC headache medicine’ was the most common reason for hesitating to visit a doctor (34.9%), even among respondents with ≥ 10 monthly days of OTC drug use (44.5%) (Table 5). Even though respondents with ≥ 10 monthly days of OTC drug use had significant migraine burden (mean [SD] MHD 11.5 [9.0]; Additional file 4), approximately 30% of these respondents responded, ‘Even after consulting, I was only prescribed medication similar to OTC headache medicine’ and ‘I thought there wouldn’t be better treatments or remedies than what I was already using.’
Among 4605 respondents who answered that they communicated with doctors in the past year, 14.6% spoke about OTC drug use and 12.5% spoke about new treatments in their consultations with the doctors. This proportion increased to 27.2% and 19.1% in respondents with ≥ 10 monthly days of OTC use.
Discussion
This real-world analysis of OTC drug use in Japanese respondents with migraine described the challenges they potentially face in accessing appropriate medical management. The study highlighted that nearly three-fourths of the respondents with migraine used OTC drugs in the past year, irrespective of the number of MHDs. Most respondents (79.0%) used OTC drugs more than prescribed acute drugs, although this proportion reduced with an increase in the number of MHDs. More than one-third of the respondents answered that they would usually use OTC drugs in addition to prescribed acute drugs when they had migraine attacks. This may increase the risk of MOH unless a doctor is aware of the OTC drug use and manages the prescribed acute drug use accordingly. Compared with the overall population, the use of OTC drugs was less among respondents who consulted doctors for migraine in the past year; however, the overall trend regarding frequent OTC drug use was still observed. Only 14.6% of respondents with migraine discussed OTC drugs with their doctors; access and awareness about migraine-specific prescription drugs were also limited.
The high prevalence of OTC drug use observed in this study (72.7%) is consistent with previous OVERCOME studies from Japan (75.2%) [4], the EU (70.5%) [23], and the US (81.8%) [18]. In the current study, the prevalence of OTC drug use was also high (65.6%) among respondents who consulted doctors over the past year. NSAIDs and triptans were the most commonly prescribed acute drugs in the current study, in line with previous Japanese studies [4, 10].
Compared with the overall population, in the subpopulation of respondents who consulted doctors for migraine in the past year, prescribed acute and preventive drug use increased, while OTC drug use decreased. This is expected, as prescribed acute and preventive drugs will only be dispensed with a doctor’s prescription. Although 62.3% of this subpopulation would usually use prescribed drugs for migraine attacks, 31.3% of them would use OTC drugs in addition to prescribed drugs, similar to a previous Japanese real-world study (31.8%) [24]. The consulting doctors may not be aware of such concomitant use of OTC and prescription drugs. More specifically, in the current study, among respondents who would usually use prescribed NSAIDs, more than one-third would also use NSAID-containing OTC drugs. This is concerning as such medication overuse may lead to MOH [9].
When the respondents were grouped by monthly days of OTC drug use, there was a notable trend: respondents with ≥ 10 monthly days of OTC drug use were diagnosed with migraine the earliest in life (mean age 25.1 years). The previous report from the OVERCOME (Japan) 2nd study (i.e., the current study), reported that OTC drugs were the first medications respondents took for their headaches (at a mean age of 19.4 years) after they started experiencing headaches (at a mean age of 17.8 years) [14]. This is likely due to the easier access for OTC drugs compared to prescription drugs. Overall, these results suggest that long-term use of OTC medications by people who started experiencing migraine at a younger age may have led to frequent use of those medications by the time of the survey i.e., later in life. Moreover, respondents with ≥ 5 monthly days of OTC drug use had numerically more MHDs and greater migraine-related burden than respondents with ≤ 4 monthly days of OTC drug use, suggesting that current medications may be inadequate to meet the needs of people with severe migraine. We also report this in Fig. 2, where both prescribed acute drug use and OTC drug use tended to be greater among respondents with more MHDs.
Since only 14.6% of respondents with migraine and 27.2% of those with ≥ 10 monthly days of OTC drug use discussed OTC drug use with doctors in the current study, doctors might be unaware of concurrent prescribed acute and OTC drug use. Additionally, claims databases, which are increasingly commonly used for medical research, also do not capture OTC drug use [10]. These highlight the challenges doctors face during consultations in accurately capturing OTC drug use by the patients and underscore the importance of careful doctor-patient communication to understand the status of patients concerning their drug treatment. Furthermore, ≥ 73.1% of respondents were unaware of migraine-specific drugs, probably because they did not communicate about new treatments with their doctors. In fact, only 12.5% of respondents spoke about new treatments with their doctors. This can partly be due to the unfamiliarity of migraine-specific drugs among consulting doctors, especially general practitioners [25, 26]. Since people with migraine mostly consult general practitioners in the real world [4, 18, 23], non-specialist doctors also play an important role in the medical management of migraine. In our previous report from the OVERCOME (Japan) 2nd study, the respondents received migraine-specific drugs such as triptans more than a decade after headache onset [14]. This indicates the need for non-specialist doctors such as general practitioners to be educated about migraine and consider referral to a specialist if required [27, 28], thus reducing the time taken for treatment and decreasing patient burden [29].
Approximately half of the respondents with ≥ 5 monthly days of OTC drug use hesitated to visit doctors because they thought they could handle the headaches with OTC drugs. Other reasons for hesitation, such as “I thought I didn’t need to go to the hospital for just a headache” and “I thought the doctor wouldn’t understand the severity or anxiety of my headache,” which were highest in the ≥ 10 monthly days of OTC drug use subgroup, have also been reported before [30,31,32]. Reasons for hesitation such as ‘Even after consulting, I was only prescribed medication similar to OTC headache medicine’ and ‘I thought there wouldn’t be better treatments or remedies than what I was already using’ suggest that approximately 30% of respondents in the ≥ 10 monthly days of OTC drug use subgroup may have been unaware of the potential benefit of migraine-specific drugs. Despite such hesitations, people in the ≥ 10 monthly days of OTC drug use subgroup experienced an average of 11.5 MHDs. It is possible that the Japanese cultural belief in ‘gaman’, i.e., ‘perseverance,’ ‘tolerance,’ or ‘self-denial,’ leads them to fight through the migraine-related burden in their daily lives and deprioritize their migraine management as much as possible [30]. However, poor migraine management can increase absenteeism and presenteeism [4, 30], negatively impact work productivity [4, 30], and add to migraine-related costs [33]. To prevent this burden, patient education is necessary. This involves increasing awareness about the risks of not seeking appropriate medical care (such as MOH and progression to CM), informing patients about the disease and cutting-edge treatment options, counseling them about realistic treatment expectations, and providing guidance on accessing suitable treatment centers [31, 34, 35].
The prevalence rate of probable MOH in the current study (2.6%) was consistent with that of previous Japanese studies (2.3–3.7%) [7, 10]. By definition, MOH can only be diagnosed in individuals with ≥ 15 MHDs [9], however, medication overuse per ICHD-3 criteria [9] can occur in individuals with < 15 MHDs too. Real-world studies from the EU [36] and the US [37] reported a medication overuse prevalence of 10.7–17.7%; respondents had an average of 11.2–12.1 MHDs. Furthermore, respondents with medication overuse had greater disease burden and healthcare resource utilization than those without medication overuse [36, 37]. The current study did not assess medication overuse prevalence; however, 29.6% of respondents with ≥ 10 monthly days of OTC drug use had probable MOH, suggesting that medication overuse, especially in this subgroup, may be high.
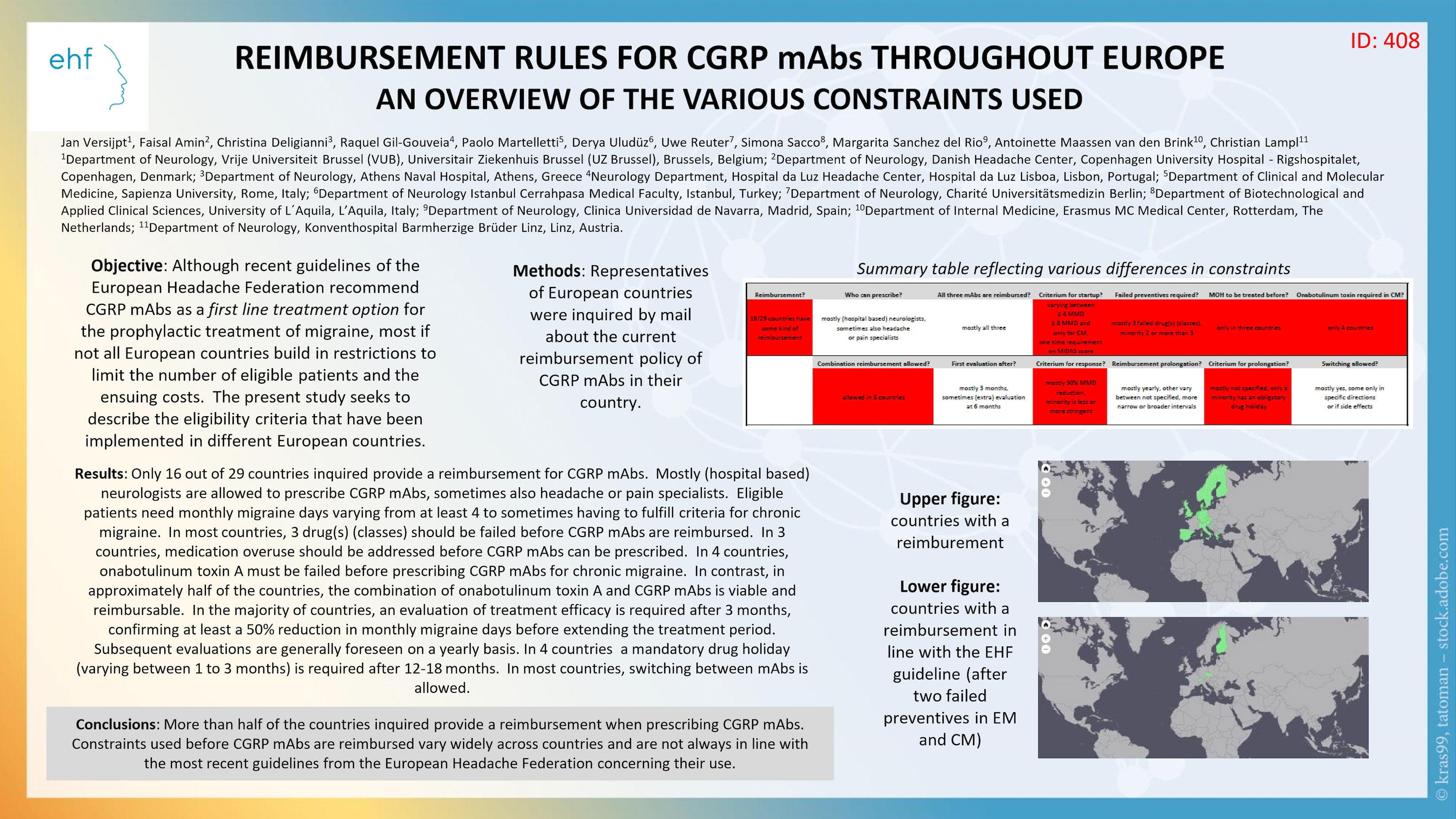
Medication overuse is associated with the risk of migraine progression from episodic migraine to CM [38,39,40]. Hence, it is essential for doctors to actively communicate with patients about OTC drug usage, educate them about medication overuse and MOH, and provide appropriate medical intervention if required [41]. Among new migraine medications, CGRP mAbs reduced MHDs in patients with MOH by 22.7% after a month’s treatment [42]. This suggests that CGRP mAbs may be a viable treatment option for individuals with MOH. However, treatment with CGRP mAbs is expensive [43], so patients need to meet certain criteria to receive reimbursement before receiving treatment. In Japan, CGRP mAbs are recommended for and reimbursed for patients who experience ≥ 4 monthly migraine days and ≥ 1 oral preventive treatment failure [44]. Basically, patients have to pay 30% of the cost and the rest is covered by Japan’s national health insurance [44]. Reimbursement criteria also vary widely in Europe [45]. However, the criteria are much more stringent in the US [46], and the insurance coverage depends on the patient’s insurance plan and the insurance company’s reimbursement criteria [44]. Issues such as delays and denials in obtaining prior authorization, non-medical switching, and lack of coverage for combination therapy also impact patient access to appropriate treatment [47]. A recent change in German reimbursement policy allowed erenumab prescriptions for patients with migraine who failed one preventive medication [48]. This led to a significantly greater reduction in MHD and an increase in ≥ 50% response rate compared with patients treated per the previous policy. Similar studies in other countries could generate evidence supporting early initiation of CGRP mAbs in the course of migraine progression and thus increase patient access to these medications.
Strengths and limitations
Danno et al. [14] describes the strengths and limitations of the OVERCOME (Japan) 2nd study. Describing the medical management of migraines and patient attitudes towards migraines by monthly use of OTC drug subgroups is a major strength of the current analysis because capturing this information through medical consultations is difficult for doctors. Such data may be helpful to alter migraine management based on an individual’s monthly use of OTC drugs. This analysis has some limitations too. Due to its online nature, the study only included participants with internet access. To assess the monthly use of drugs, days of individual drug use were summed up for each drug class (prescribed acute or OTC drugs), so we may have overestimated the number of days when multiple drugs were used in combination on the same day. Respondents self-reported the data so we cannot rule out recall bias. The current survey included similar or common questions as the previous OVERCOME (Japan) study in 2020 [4], but some questions were newly created for the current survey or adapted from previous OVERCOME studies [17, 18]. Such questions may not have been validated in the Japanese population.
Conclusion
The current analysis of the OVERCOME (Japan) 2nd study shows that OTC drug use is common among respondents with migraine, regardless of the number of MHDs, and even among those who have consulted doctors and are on prescribed acute drugs. Some respondents even use OTC drugs more frequently than or along with prescribed acute drugs. OTC drug use is not commonly discussed during consultations. Moreover, the majority of the respondents, even those who were consulting doctors or with frequent OTC drug use, did not have access to or awareness of migraine-specific drugs. Respondents also did not prioritize migraine management. Therefore, to prevent MOH, doctors should communicate with patients about OTC drug use, treat them with appropriate prescription drugs, and provide adequate information and medical intervention.
Data availability
The datasets generated and/or analyzed during the current study are available at Eli Lilly Japan K.K on reasonable request.
Abbreviations
- CGRP mAbs:
-
Calcitonin Gene-related Peptide Monoclonal Antibodies
- CM:
-
Chronic Migraine
- HIT:
-
6-Headache Impact Test-6
- ICHD:
-
3-International Classification of Headache Disorders-3rd edition
- MHD:
-
Monthly Headache Days
- MIBS:
-
4-Migraine Interictal Burden Scale-4
- MIDAS:
-
Migraine Disability Assessment Scale
- MOH:
-
Medication Overuse Headache
- OTC:
-
Over-the-counter
- OVERCOME:
-
ObserVational survey of the Epidemiology, tReatment, and Care Of MigrainE
- PRO:
-
Patient-reported Outcomes
References
Takeshima T, Ishizaki K, Fukuhara Y, Ijiri T, Kusumi M, Wakutani Y, Mori M, Kawashima M, Kowa H, Adachi Y et al (2004) Population-based door-to-door survey of migraine in Japan: the Daisen study. Headache 44:8–19
Sakai F, Igarashi H (1997) Prevalence of migraine in Japan: a nationwide survey. Cephalalgia 17:15–22
Institute of Medical Studies (2021) Headache Practice Guidelines 2021 [in Japanese]. 512 p. Available from: https://www.neurology-jp.org/guidelinem/pdf/headache_medical_2021.pdf
Hirata K, Ueda K, Komori M, Zagar AJ, Selzler KJ, Nelson AM, Han Y, Jaffe DH, Matsumori Y, Takeshima T (2021) Comprehensive population-based survey of migraine in Japan: results of the observational survey of the epidemiology, tReatment, and care of migraine (OVERCOME [Japan]) study. Curr Med Res Opin 37:1945–1955
Ravishankar K (2008) Medication overuse headache in India. Cephalalgia 28:1223–1226
Takeshima T, Ueda K, Komori M, Zagar AJ, Kim Y, Jaffe DH, Matsumori Y, Hirata K (2022) Potential unmet needs in acute treatment of migraine in Japan: results of the OVERCOME (Japan) study. Adv Ther 39:5176–5190
Katsuki M, Yamagishi C, Matsumori Y, Koh A, Kawamura S, Kashiwagi K, Kito T, Entani A, Yamamoto T, Ikeda T, Yamagishi F (2022) Questionnaire-based survey on the prevalence of medication-overuse headache in Japanese one city-Itoigawa study. Neurol Sci 43:3811–3822
Alshareef M (2022) Factors associated with Over-the-Counter analgesic overuse among individuals experiencing headache. Clin Pract 12:714–722
(2018) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38:1-211
Takizawa T, Kitano T, Iijima M, Togo K, Yonemoto N (2024) Treatment patterns and characteristics of patients with migraine: results from a retrospective database study in Japan. J Headache Pain 25:19
Sleath B, Rubin RH, Campbell W, Gwyther L, Clark T (2001) Physician-patient communication about over-the-counter medications. Soc Sci Med 53:357–369
Kotani K, Shimomura T, Ikawa S, Sakane N, Ishimaru Y, Adachi S (2004) Japanese with headache: suffering in silence. Headache 44:108–109
Pharmaceuticals and Medical Devices Agency (2024) List of Approved Drugs April 2004 to January 2024. Available via https://www.pmda.go.jp/files/000272313.pdf. Accessed March 03, 2025
Danno D, Suzuki S, Takizawa T, Ishii R, Hamakawa M, Tanizawa Y, Osaga S, Komori M (2025) The impact of migraine on the whole life course of patients: results from the OVERCOME (Japan) 2nd study. Neurol Ther 14:335–356
Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M (2001) Prevalence and burden of migraine in the united States: data from the American migraine study II. Headache 41:646–657
Silberstein S, Loder E, Diamond S, Reed ML, Bigal ME, Lipton RB, Group AA (2007) Probable migraine in the united States: results of the American migraine prevalence and prevention (AMPP) study. Cephalalgia 27:220–229
Pascual J, Panni T, Dell’Agnello G, Gonderten S, Novick D, Evers S (2023) Preventive treatment patterns and treatment satisfaction in migraine: results of the OVERCOME (EU) study. J Headache Pain 24:88
Lipton RB, Nicholson RA, Reed ML, Araujo AB, Jaffe DH, Faries DE, Buse DC, Shapiro RE, Ashina S, Cambron-Mellott MJ et al (2022) Diagnosis, consultation, treatment, and impact of migraine in the US: results of the OVERCOME (US) study. Headache 62:122–140
Iigaya M, Sakai F, Kolodner KB, Lipton RB, Stewart WF (2003) Reliability and validity of the Japanese migraine disability assessment (MIDAS) questionnaire. Headache 43:343–352
Kosinski M, Bayliss MS, Bjorner JB, Ware JE Jr., Garber WH, Batenhorst A, Cady R, Dahlof CG, Dowson A, Tepper S (2003) A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res 12:963–974
Buse D, Bigal MB, Rupnow M, Reed M, Serrano D, Lipton R (2007) Development and validation of the migraine interictal burden scale (MIBS): A self-administered instrument for measuring the burden of migraine between attacks. Neurology 68:A89
Buse DC, Rupnow MF, Lipton RB (2009) Assessing and managing all aspects of migraine: migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin Proc 84:422–435
Evers S, Dell’Agnello G, Novick D, Gonderten HS, Panni T, Pascual J (2024) Acute treatment patterns, migraine burden, and healthcare resource use in people with migraine: results from the OVERCOME (EU) observational study. Pain Ther 13:589–607
Sakai F, Hirata K, Igarashi H, Takeshima T, Nakayama T, Sano H, Kondo H, Shibasaki Y, Koga N (2022) A study to investigate the prevalence of headache disorders and migraine among people registered in a health insurance association in Japan. J Headache Pain 23:70
Takaki H, Onozuka D, Hagihara A (2018) Migraine-preventive prescription patterns by physician specialty in ambulatory care settings in the united States. Prev Med Rep 9:62–67
Fathy M, ElSadek A, Farag S, Helmy S, AbdElMoneim A (2021) Dilemma of migraine diagnosis and management among non-neurologists. Egypt J Neurol Psychiatry Neurosurg 57:118
Beithon J, Gallenberg M, Johnson K, K P, Liebow JK, Linbo M, Myers L, Peterson C, Schmidt S, Swanson J J. Diagnosis and treatment of headache: health care guideline. Bloomington, MN: Institute for Clinical Systems Improvement; 2013 December 19, 2024]. Available from: https://www.icsi.org/guidelines__more/catalog_guidelines_and_more/catalog_guidelines/catalog_neurological_guidelines/headache/
Dougherty C, Silberstein SD (2015) Providing care for patients with chronic migraine: diagnosis, treatment, and management. Pain Pract 15:688–692
Vaghi G, De Icco R, Tassorelli C, Goadsby PJ, Vicente-Herrero T, de la Torre ER (2023) Who cares about migraine? Pathways and hurdles in the European region - access to care III. J Headache Pain 24:120
Matsumori Y, Ueda K, Komori M, Zagar AJ, Kim Y, Jaffe DH, Takeshima T, Hirata K (2022) Burden of migraine in Japan: results of the observational survey of the epidemiology, tReatment, and care of migraine (OVERCOME [Japan]) study. Neurol Ther 11:205–222
Karasawa Y, Yamaguchi K, Nakano S, Nozawa K, Iseki M (2023) Barriers to healthcare access in patients with chronic pain or potential migraine in Japan: a cross-sectional internet survey. Front Pain Res (Lausanne) 4:1271438
Pascual J, Nunez M, Panni T, Diaz-Cerezo S, Novick D, Ciudad A (2023) Burden and unmet needs in migraine patients: results from the OVERCOME (Spain) study. Pain Ther 12:1209–1220
Shimizu T, Sakai F, Miyake H, Sone T, Sato M, Tanabe S, Azuma Y, Dodick DW (2021) Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J Headache Pain 22:29
Igarashi H, Komori M, Ueda K, Zagar AJ, Jaffe DH, Matsumori Y, Takeshima T, Hirata K (2024) Underrecognition of migraine-related stigmatizing attitudes and social burden: results of the OVERCOME Japan study. Brain Behav 14:e3547
Igarashi H, Sano H, Kondo H, Shibasaki Y, Koga N (2024) Characteristics of patients who seek medical attention for headache and those who do not: cross-sectional survey and linked medical claims data analysis in Japan. BMJ Open 14:e077686
Dissing AS, Lee XY, Osterberg O, Hammer-Helmich L (2023) Burden of medication overuse in migraine: A Cross-sectional, Population-Based study in five European countries using the 2020 National health and wellness survey (NHWS). Neurol Ther 12:2053–2065
Schwedt TJ, Buse DC, Argoff CE, Reed ML, Fanning KM, Hussar CR, Adams AM, Lipton RB (2021) Medication overuse and headache burden: results from the cameo study. Neurol Clin Pract 11:216–226
Buse DC, Greisman JD, Baigi K, Lipton RB (2019) Migraine progression: A systematic review. Headache 59:306–338
Lipton RB, Serrano D, Nicholson RA, Buse DC, Runken MC, Reed ML (2013) Impact of NSAID and Triptan use on developing chronic migraine: results from the American migraine prevalence and prevention (AMPP) study. Headache 53:1548–1563
Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB (2008) Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache 48:1157–1168
Vandenbussche N, Laterza D, Lisicki M, Lloyd J, Lupi C, Tischler H, Toom K, Vandervorst F, Quintana S, Paemeleire K, Katsarava Z (2018) Medication-overuse headache: a widely recognized entity amidst ongoing debate. J Headache Pain 19:50
Ito Y, Mitsufuji T, Okada M, Fujita S, Yokoyama R, Kawasaki H, Yamamoto T (2023) Early effect of calcitonin Gene-related peptide monoclonal antibodies in migraine with medication overuse: A Single-center retrospective study. Intern Med 62:3455–3460
Varnado OJ, Manjelievskaia J, Ye W, Perry A, Schuh K, Wenzel R (2022) Health care resource utilization and costs associated with treatment among patients initiating calcitonin gene-related peptide inhibitors vs other preventive migraine treatments in the united States. J Manag Care Spec Pharm 28:818–829
Takizawa T, Ihara K, Watanabe N, Takemura R, Takahashi N, Miyazaki N, Shibata M, Suzuki K, Imai N, Suzuki N et al (2024) CGRP-monoclonal antibodies in Japan: insights from an online survey of physician members of the Japanese headache society. J Headache Pain 25:39
Versijpt J, Amin F, Deligianni C, Gil-Gouveia R, Martelletti P, Uluduz D, Reuter U, Sacco S, Sanchez del Rio M, van den Brink AM, Lampl C (2023) Reimbursement rules for CGRP mAbs throughout Europe. An overview of the various constraints used. Available via https://www.cgrpforum.org/wp-content/uploads/Reimbursement-Europe.jpg. Accessed March 12, 2025
American Headache Society (2019) The American headache society position statement on integrating new migraine treatments into clinical practice. Headache: J Head Face Pain 59:1–18
Insurance’s Impact on Patient Access to Migraine Treatment (2025) Available via https://static1.squarespace.com/static/5886319ba5790a66cf05d235/t/65f9fc4ec4e17d65f19b48c3/1710881873681/SurveySummaryReportMM-HMPF-March2024.pdf. Accessed March 12
Hong JB, Lange KS, Fitzek M, Overeem LH, Triller P, Siebert A, Reuter U, Raffaelli B (2023) Impact of a reimbursement policy change on treatment with erenumab in migraine – a real-world experience from Germany. J Headache Pain 24:144
How to Choose Over-the-Counter Pain Relievers and Fever Reducers (2025) Available via https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00404.html. Accessed March 26
Acknowledgements
Leo J. Philip Tharappel of Eli Lilly Services India Private Limited, Bengaluru, India, provided medical writing and editorial support, which Eli Lilly Japan K.K funded.
Funding
Eli Lilly Japan K.K. funded this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conceptualization, investigation, and methodology. All authors reviewed and approved the submitted version and agreed to be accountable for their contributions. MM performed data collection and statistical analyses. YT supervised the study and disclosure development and drafted the disclosure. MK supervised the study.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Medical Corporation TOUKEIKAI Kitamachi Clinic ethics committee approved this study (number BGQ09531) on April 19, 2023. This study was conducted per ethical principles originating from the Declaration of Helsinki and that was consistent with Good Pharmacoepidemiology Practices. All applicable Japanese laws and regulations were followed. All survey respondents provided electronic informed consent and agreed to participate in the study. All data were anonymized before analysis.
Consent for publication
Not applicable.
Competing interests
RI received consulting fees from Amgen K.K., Eli Lilly Japan K.K., Daiichi Sankyo Co., Ltd., and Otsuka Pharmaceutical Co., Ltd; speaker honoraria from Amgen K.K., Daiichi Sankyo Co., Ltd., and Otsuka Pharmaceutical Co., Ltd. TT is a consultant/advisor and/or serves on an advisory board for Eli Lilly Japan K.K., Otsuka Pharmaceutical Co., Ltd., Amgen K.K., Pfizer Japan Inc., and Teijin Pharma Ltd. He received speaker honoraria from Eli Lilly Japan K.K., Daiichi Sankyo Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Amgen K.K., Kowa Company, Ltd., Kyowa Kirin Co., Ltd., Eisai Co., Ltd., UCB Japan Co., Ltd., Takeda Pharmaceutical Company Ltd., and Santen Pharmaceutical, a grant from Pfizer Japan Inc., and research funding from Eli Lilly Japan K.K. and Tsumura & Co., outside the submitted work. SS received speaker honoraria from Amgen K.K., Daiichi Sankyo Co., Ltd., Eli Lilly Japan K.K., and Otsuka Pharmaceutical Co., Ltd. DD serves on the advisory boards of and received speaker honoraria from Amgen K.K., Daiichi Sankyo Co., Ltd., Eli Lilly Japan K.K., and Otsuka Pharmaceutical Co., Ltd. MM is an employee of Social Survey Research Information Co., Ltd. Social Survey Research Information Co., Ltd. performed data collection and statistical analyses in this study and was sponsored by Eli Lilly Japan K.K. YT, SO, CH, and MK are employees of Eli Lilly Japan K.K. and may own stock/stock options of Eli Lilly and Company.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Ishii, R., Takizawa, T., Suzuki, S. et al. Real-world use of over-the-counter medications by patients with migraine in Japan: results from the OVERCOME (Japan) 2nd study. J Headache Pain 26, 107 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s10194-025-02046-8
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s10194-025-02046-8